Synthetic alternatives to donor blood have been stuck in development for decades. Nina Notman reports on recent promising progress
Synthetic alternatives to donor blood have been stuck in development for decades. Nina Notman reports on recent promising progress
Human blood substitutes have been in the pipeline since the 1980s. But, for a combination of scientific and political reasons, there are none currently on the market in either Europe or the US. There are a few blood substitutes still progressing through clinical trials, and the academic community is still actively improving the products, also known as oxygen therapeutics and haemoglobin-based oxygen carriers.

’No one was interested in this type of work until HIV came in the 1980s,’ explains Thomas Chang from McGill University, Montreal, Canada, an early pioneer of the field, ’and then everyone started to look into making artificial blood substitutes.’
He adds, ’we have to be ready for another HIV episode or similar when the blood might be contaminated.’ It was HIV concerns that led to South Africa becoming one of the few countries so far to approve the use of a blood substitute - a product called Hemopure.
Fears of contaminated donor blood supplies are just one reason for the interest in this area. Ongoing concerns about lack of donor blood supplies in remote locations are also driving the field forward, with the US army and navy funding much of the research. You never know when there will be a disaster or war when we won’t have sufficient blood reserves, says Chang. More niche needs include patients, such as Jehovah’s Witnesses, who for religious reasons can not use donor blood, and patients who have developed immune responses to donated blood.
Aside from not being reliant on donor blood supplies, other major advantages of artificial blood include not needing to check blood types before transfusion - artificial blood is the universal blood group O negative. Artificial blood also avoids shelf life issues - donor blood can be stored for a maximum of 42 days before use, and starts to degrade in quality shortly after collection.
Outsmarting obstacles
The need and utility may be clear, but the route to regulatory approval in Europe and the US has been tortuous - with numerous hurdles seemingly intent on blocking the way.
The first clinical trials for these products - run by a number of different companies - had disappointing results with some unwanted side effects, most seriously an increase in blood pressure. Chang blames the results on a rush to get a product to market in the wake of the HIV crisis: ’not enough basic research was done prior to HIV - and as a result, when it was realised that donor blood could be contaminated, companies started to make many different types of blood substitutes, and unfortunately some don’t work and some have adverse side effects.’
The concerns came to a head in early 2008, when a meta-analysis of findings from 16 clinical trials of five different products that had been used on over 3500 patients was published in the Journal of the American Medical Association . The study, led by Charles Natanson, a senior scientist at the US National Institutes of Health, revealed a threefold increase in the risk of heart attacks in patients who received the substitutes, compared with the control group who received donor blood (see Chemistry World , June 2008, p13).
’The paper by Natanson combined the results of all the clinical trials, of all the products, from all the companies, and lumped them together,’ says Chang, ’and that was a disaster for this field.’ Some of the products had fewer side effects than others, but because they were treated as one everyone started to worry and the US Food and Drug Administration (FDA) became reluctant to approve anything, he says.
Chang’s frustration is shared by many scientists working in the field, including John Olson, based at Rice University, Houston, US: ’the Natanson article says every blood substitute is evil and causes heart attacks. But like everything in science, it is how you package the data for presenting.’
Natanson, however, stands by his findings: ’meta-analysis showed that if you put all the studies together there was a very common toxicity - that is they appeared to cause heart attacks and death.’ It appeared to be a very consistent finding no matter what type of patients you were looking at or which of the various companies you looked at, he adds.
Hemopure
Although the FDA is currently wary of these products, a handful of companies in the US are still working their way through the obstacles in the attempt to get a blood substitute to market.
According to Olson, the best of the bunch is Hemopure - a blood substitute being developed by the oxygen therapeutics firm OPK Biotech. Hemopure was initially designed by the small start up company Biopure, which was brought by OPK Biotech when it went bankrupt last year (see Chemistry World, 14 May 2009.
’Hemopure is the one, in my opinion, that should be closest to being approved for use when no donated blood is available,’ Olson says. ’It is the simplest and the cheapest technology.’
As Rick Light, vice president of research and development at OPK Biotech, explains: ’an important distinction between Hemopure and any other haemoglobin-based oxygen carrier is that Hemopure is room temperature stable as a liquid for at least 3 years.’ You just pull it off the shelf and use it immediately, he says. This stands it apart from other potential blood substitutes that need refrigeration, or are freeze-dried, meaning they have to be reconstituted with plasma.
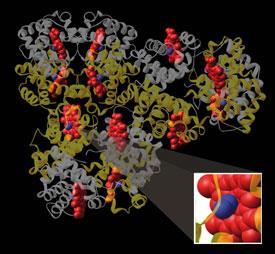
To make Hemopure ’we take bovine blood and, using filtration and chromatography, purify the haemoglobin so it is 99.9 per cent pure protein,’ explains Light. But sadly it isn’t as simple as just dissolving the haemoglobin in a fluid and transfusing it into the patient. Native haemoglobin is tetrameric and dissociates into dimers in the body that are excreted through the kidneys with a half life of about 30 minutes. ’Which is not a very effective therapy,’ Light points out. ’You have to modify the haemoglobin so it doesn’t dissociate.’
A number of different approaches have been taken to stop this dissociation. ’What we do is polymerise with glutaraldehyde [pentane-1,5-dial] to make large polymers of haemoglobin that have a half life of between 18 and 24 hours in the body,’ Light says.
The polymerised haemoglobin is then put into a physiological buffer, which contains salts and lactates to maintain heart function. At this stage the product still contains about 30 per cent stabilised haemoglobin tetramers - and while they may not dissociate in this form, they are still problematic because they can enter blood vessel walls and scavenge nitric oxide. NO naturally causes the walls of blood vessels to relax, so if too much NO is scavenged, relaxation is prevented, making it more difficult for blood to flow, resulting in an increase in blood pressure. A final clean up stage removes most of the tetramer haemoglobin, significantly reducing the blood pressure effect, explains Light.
Once transfused into the body, polymerised haemoglobin works in the same way as a red blood cell: it binds to oxygen in the lungs, carries it to the appropriate site in the body and then releases it. What makes it different to red blood cells is that the haemoglobin is free in the plasma - rather than bound within the cell.
The advantage of the haemoglobin being in the plasma is that the oxygen it carries is closer to the sides of blood vessels. Oxygen binding and release in the plasma is more efficient than in the red cell, says Light, so Hemopure releases oxygen more quickly than donor blood once it gets to the target tissue. At end of its life, Hemopure is broken down by the normal biological pathway for haemoglobin.
Hemopure is currently approved for use in South Africa, and has undergone some early clinical trials in the US. Production stopped, however, when Biopure went bankrupt - and OPK Biotech is currently focusing on getting production back online. Referring to the FDA’s concerns over these products, Light predicts that they will be approved overseas before approval in the US. The firm’s parent company, OPK, is Russian and, according to Light, ’OPK have a great interest in bringing this product to Russia.’
MP4
Another, slightly different, product making its way through clinical trials in Europe is Sangart’s MP4. ’Our agent is given together with blood to improve the oxygen transfer to tissues from red cells,’ explains Howard Levy, chief scientific officer for the San Diego-based firm.
MP4 is transfused into patients in an approximately 1:19 MP4:donor blood ratio. Explaining the need for his product, Levy says: ’the trouble is [when] blood is stored for long periods; beyond 3 days it undergoes changes that make it less efficient at delivering oxygen.
’MP4 first releases its own oxygen, and is then able to take oxygen from red cells and give it to tissues,’ he adds.
Clinical trials in Europe with this product are progressing well. ’We have just completed a Phase II trauma study,’ says Levy. ’So we are in the process of cleaning the database and will then proceed to analyse the data.’ He adds: ’we’re looking for market launch at the end of 2013 or the beginning of 2014.’
The haemoglobin for MP4 comes from out-of-date human blood, rather than the bovine blood used for Hemopure. And to prevent tetramer toxicity and dissociation, Sangart takes the alternative approach of coating the haemoglobin with polyethylene glycol (PEG).
’2-Iminothiolane is added to haemoglobin to increase the number of thiol sites on the molecule. And then PEG is able to attach to these thiol sites,’ Levy explains.
As well as coating the molecule, PEG binds next to haemoglobin’s oxygen binding site - altering the way oxygen attaches and detaches from the molecule. ’It very much increases the affinity of oxygen, so that oxygen is held on very, very tightly and only released if it reaches the level in the tissues where there is an oxygen lack,’ Levy says. And this is one of the key selling points of MP4, according to Levy: that it delivers oxygen exactly where it is needed in the body.
Blood pharming
Another potential route to blood substitutes is to grow human red blood cells from cells extracted from umbilical cords - a technique called blood pharming.
One biotechnology firm exploring this approach is Arteriocyte, based in Cleveland, US. ’We have demonstrated proof of concept that we can take umbilical cord cells, expand them and differentiate them [into red blood cells] in useful volumes,’ says Adam Sorkin, Arteriocyte’s director of research and development.
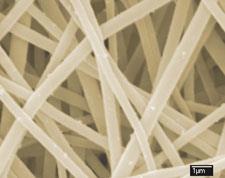
The first step is to isolate haematopoietic stem cells from an umbilical cord. ’We then culture those on our Nanex technology, which is a polymer nanofibre substrate that expands the stem cells much more rapidly than normal cell culture techniques,’ Sorkin explains. ’In 10 days we get a 300 to 350-fold increase in cells and over a month we can get hundreds of thousands, or a million-fold increase.’
The second stage is to recreate the differentiation process that occurs normally in the body, in vitro. ’Using a special cocktail of growth factors that we change over the course of several weeks, we gradually drive most of these stem cells to form red blood cells that are functionally indistinguishable from the red blood cells you would produce natively.’
Finally, the cells are filtered and put in plasma or fluid before they can be transfused directly into the body.
The end goal is to carry out the complete process onsite in remote areas such as in hospitals in war zones. ’Once it’s up and running, the idea is that it will be producing universal donor blood on demand,’ says Sorkin.
’What we are working on now is implementing the bioreactor technology that will handle the differentiation step. At that point we would move into [clinical] trials.’ Sorkin predicts that it will take another 5-10 years for this product to reach the market.
Academic interest
While it looks hopeful that these blood substitutes may eventually make it to market in Europe and the US, many others have failed during the development or clinical trials phases - including Northfield Laboratories’ Polyheme and Baxter’s Rhb2.0.

’We definitely have to look seriously into new generations of blood cell substitutes to solve some of the problems and ensure that there are no side effects at all in future blood substitutes,’ says Chang at McGill University. Chris Cooper, an expert in haemoglobin at the University of Essex, UK, agrees: ’The blood substitute field has in a sense gone back to the academics for the moment.’
In the quest to find this next generation blood substitute, Cooper and Rice University’s Olson - among others - are studying the fundamentals of how haemoglobin works to figure out what causes the increase in blood pressure.
The observation that tetramers scavenge NO is a well known cause of haemoglobin’s toxicity outside of red blood cells, initially uncovered by Olson, but more recently Cooper has suspected a multifactorial cause. In 2008, Cooper and his team published a paper in the Journal of Biological Chemistry demonstrating that a previously unknown electron transfer pathway in haemoglobin is partly key to the toxicity problem. ’Haemoglobin reacts with peroxides [naturally present in the body] and creates toxic free radicals,’ says Cooper. ’So what we’ve done is look at these electron transfer pathways and engineer around them.’
The team found that there are residues of the amino acid tyrosine within haemoglobin’s structure and adding more - using protein engineering - allows the body to better defend against free radical attack.
Olson, whose Rice-based team is also looking at bioengineering haemoglobin, explains, ’we can look at the molecule like an engineer looking at an internal combustion machine and say "how can I engineer this to work better?"’
Both Olson and Cooper grow their modified human haemoglobin in Escherichia coli . ’It’s a great idea in principle; all you need is corn syrup, minerals and bacteria to have continuous production of haemoglobin using conventional manufacturing standards,’ says Olson.
’We can change the programme for making haemoglobin by selectively changing amino acids, to try to get rid of any side effects or to optimise it for better transport,’ he adds. His team is currently making adaptations to improve shelf life and efficiency.
Artificial red blood cell
The toxicity problems that plague blood substitutes are believed to originate from the free tetrameric haemoglobin in the products, and an alternative approach being considered is to encase the tetramers in an artificial container - in essence mimicking the red blood cells.

One researcher working in this field is Thomas Chang from McGill University, Montreal, Canada. ’The artificial red blood cell contains a membrane or polymer [casing] around the haemoglobin,’ he explains. The casing is made from biodegradable polymers, such as poly(lactic acid), that degrades into lactic acid and then water and carbon dioxide in the body. Inside his ’cell’, Chang has also included two enzymes - catalase and superoxide dismutase - that remove toxic radicals in a further attempt to recreate conditions similar to the natural cell.
’The artificial cell is about 80nm in diameter, 100 times smaller that natural red cells,’ says Chang. Initial animal tests have been encouraging, showing no adverse effect on the function of the liver or spleen. The artificial cells also stay circulating in the body’s blood supply for twice as long as the polymerised haemoglobin products. ’It looks promising and we are continuing researching this,’ says Chang.
Weighing up costs
The E. coli approach is appealing as it avoids the need for supplies of either human or bovine blood - but there is a huge issue: price. ’No one has ever made E. coli technology as cheaply as we would have to make this,’ Olson explains. A unit of donor blood (60g) costs a hospital $300 (?194), meaning to match the price the product would need to be made for $6 a gram. ’For recombinant technology that’s not easy to do, we are currently at $200-1000 a gram.’
The cost issue is not unique to the E. coli approach however, with both Sangart and OPK Biotech admitting their technology is not cheap and Adam Sorkin from Arteriocyte admitting that ’cost is one of the challenges we face as we scale up our process.’
So with cost problems to add to the ever growing list of hurdles blood substitutes must jump before they make it to market - is the concept doomed to fail? No, is the resounding answer from the experts. ’It just needs one product to get on the market and then there will be an obvious market and others will take off,’ Cooper says confidently.



1 Reader's comment