Simon Hadlington previews the novel materials coming soon to a dental surgery near you
Simon Hadlington previews the novel materials coming soon to a dental surgery near you
Teeth have a hard time of things. Not only are they required to crunch, break, chew and tear, they also exist in a remarkably hostile and extremely variable environment. So when it comes to mending damaged or diseased teeth and bones in the mouth, the challenge to develop materials that can cope with these stresses are nothing if not substantial. Furthermore, there is an increasing demand from patients that materials are aesthetically pleasing - ugly metallic fillings are gradually becoming a thing of the past. The chemistry behind fixing teeth and bones in the mouth, and developing new ways to prevent damage is, literally, science at the sharp end.
’The mouth is a very dynamic environment, chemically, biologically and mechanically,’ says Jonathan Knowles, a professor of biomaterials at the renowned Eastman Dental Institute at University College London, UK. ’It poses some unique and difficult conditions. People eat ice cream and they drink tea - so you get extremes of temperature from 70?C down to zero. pH changes can be significant either locally, with bacteria producing acid, or more generally from fizzy drinks or orange juice. Then there is a strong mechanical element, with the jaw and tongue constantly moving, and with high mechanical loads applied to the teeth.’
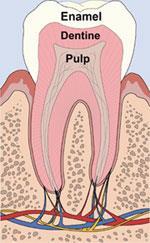
To withstand these trials, the tooth is exceptionally tough. The outer layer, enamel, is the hardest tissue in the body, consisting almost entirely of hydroxyapatite (crystalline calcium phosphate). The enamel, which can be up to 2.5mm thick in places, sits on top of dentin, which is composed mainly of hydroxyapatite and the sturdy protein collagen.
Shunning mercury
Enamel and dentin are both susceptible to acid-induced demineralisation, necessitating a filling or restoration. For more than 100 years the main material for restorations has been dental amalgam, whose current typical formulation is a mixture of around 50 per cent mercury with smaller proportions of silver, tin, copper and zinc. The advantage of amalgam is that it is relatively inexpensive and is highly durable. However, health concerns are raised periodically about the mercury content of amalgam (the dental profession is generally adamant that there is no reliable long-term evidence to support these concerns) and amalgam fillings are unsightly.
’There has been a massive decline in the use of amalgam in the west,’ says David Watts, a biomaterials expert at the University of Manchester in the UK. ’Norway has banned it, and its use has dropped massively in Germany and in the UK.’
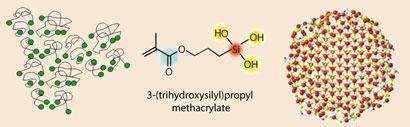
Instead, dentists are using resin composites, which can be made tooth-coloured. These resins consist of three principal components: monomers that harden to form a matrix, embedded particles such as ceramic or glass to provide hardness and reinforcement, and a coupling agent to bond the two together - often based on a silane.
A typical monomer is bis-GMA (bisphenylglycidylmethacrylate) which has a polymerisable methacrylate group at either end. The monomer can be diluted and mixed with varying proportions of fillers - which has a profound effect on the properties of the material.
The hardening, or polymerisation, of the monomer once in the mouth is usually induced using blue light to excite a photoinitiator (such as camphorquinone) contained within the mixture. The initiator first reacts with an amine, also present in the mixture, forming a pair of free radicals. These then trigger polymerisation of the methacrylate groups at the ends of the monomers - causing extensive cross-linking and the setting of the mixture.
Shrinkage laid bare
It is at this point that Watts takes an interest. ’Most modern dental materials undergo some kind of setting reaction in the mouth to harden them, where they are transformed from a paste to a solid,’ he says. ’So we have a phase transition being introduced and this usually results in a certain amount of shrinkage, which can affect the performance of the material.’
The shrinkage - typically in the range of 2 to 4 per cent - occurs because the distance between the monomers is governed by van der Waals forces, but the covalent bonds in the polymerised molecule are much shorter, he explains.
Where the composite resin is bonded to the tooth surface, shrinkage can set up stresses within the surrounding tooth as well as in the resin itself with the possibility of gaps opening up that could become populated by bacteria.
To understand at a fundamental level how shrinkage occurs and how it might be controlled, Watts is studying the kinetics of the photopolymerisation process. He has shown that the extent of shrinkage can be governed by several factors. ’The progress of the polymerisation reaction and the ultimate properties of the composite resin can be subtly modified by things such as the light irradiation regime and the ambient temperature,’ he says. ’In addition, knock-on effects to the properties are very dependent on the initial formulation and so on. We are developing new kinetic models of these phenomena, which we think will give us important new insights into how to control shrinkage and ultimately to produce more consistent and effective results.’
Sticking with it
Another problem with resin composites is that they do not bond directly to the tooth - they need to be glued in place. Traditional amalgam fillings remain in place because a cavity is excavated into the tooth by the dentist, which is shaped so that the packed amalgam cannot move. This requires an amount of healthy tooth tissue to be removed. It is far more desirable to remove only the damaged tissue - so-called minimally invasive dentistry. This needs a sound bond between the restorative material and the tooth tissue and this in turn requires an adhesive.
At the Catholic University of Leuven in Belgium, Bart van Meerbeek is investigating new adhesive compounds. ’The big issue is that we are dealing with two substrates which the adhesive needs to bond to, enamel and dentine, which are totally different in nature,’ says van Meerbeek. ’Finding a single adhesive which will make a durable bond with both surfaces is a challenge.’
The current gold standard adhesion protocol is a three-step process. First the surface is etched with a solution of phosphoric acid, creating microscopic pores in the surface of the enamel and dentine to allow the adhesive to get a grip. Next a primer is applied, consisting of functional monomers with a polymerisable group such as methacrylate on one end and a carboxylic acid or phosphate on the other. The monomers penetrate the surfaces and coat the collagen fibres of the dentin. The bonding agent, consisting of light-curable methacrylates and dimethacrylates, can then be applied, before application of the resin composite itself.
’That is the basic procedure, and one that generally works reasonably well,’ says van Meerbeek. ’But for dentists it is seen as a complicated system and they are always looking for simpler procedures to save time.’
A less laborious approach has been to produce self-etching primers, meaning the priming and etching can be done in a single step before the glue is added. Here, acidic functional groups are incorporated into the primer monomers, such as phosphates, phosphonates or carboxylic acids.
All-in-one systems of a self-priming, self-etching adhesive have also been explored, but these have proved less effective than the three-step process. ’The ideal one-step adhesive would have an acidic functionality to do some controlled etching but not too much to degrade the dentin excessively,’ van Meerbeek says. ’It would have a functionality to allow ionic bonding with the calcium of the hydroxyapatite, and a polymerisable functionality at the other end.’ The bonding on its own is not enough, so a cross-linking monomer is also needed to make a strong adhesive through polymerisation, he explains. ’Then you need a solvent so that the adhesive can be easily applied, this must evaporate as much as possible, you need a certain amount of water in the system which should also be able to disappear before polymerisation, and you need a light curing photoinitiator.’ It is, Van Meerbeek concedes, an ambitious goal.
Poor foundations
In cases where the entire tooth has been lost, including its root, an artificial tooth can be installed into the jawbone using an implant to anchor the structure into the bone. These implants are typically made from titanium which are screwed into the bone and are usually successful when inserted into sound, healthy and well-nourished bone.

However, sometimes in patients with conditions such as osteoporosis, or who have undergone radiotherapy in the jaw, or where there is a decreased blood supply, the implant does not become well integrated into the surrounding bone tissue. At the George-Augusta-University in G?ttingen, Germany, Henning Schliephake and his team are investigating new ways to improve the performance of implants in such cases.
’When the titanium is inserted it comes into contact with biological fluids containing many complex entities,’ Schliephake says. ’Proteins attach to the surface of the metal, forming a biological matrix which becomes attractive for undifferentiated bone cells to attach to, where they then differentiate into mature bone-forming cells.’ In this way, new bone meshes itself around the artificial implant. ’One way of increasing the formation of new bone and speeding up the healing process is to increase the biological signalling that makes these undifferentiated cells become bone cells,’ he says. These signalling molecules, or growth factors, consist of peptides and Schliephake’s laboratory is looking at ways of attaching artificially created growth factor peptides to the surface of the implant in such a way that the molecules retain their biological activity and are released in the vicinity of the growing bone.
The issue here is how do we attach these peptides to the surface of the titanium - which is in fact a layer of titanium oxide - in a way that allows the molecule to retain its activity and be released locally.’ One approach that seems promising is to anchor the peptide using oligonucleotide anchor strands. These strands bind to the oxide and if the peptide is equipped with a complementary nucleotide sequence, the latter can reversibly ’hybridise’ to the anchored nucleotide, allowing it to retain its structure and to become released. This system has been developed by a material science group led by Dieter Scharnweber at the University of Dresden, Germany, and is currently being evaluated in collaboration with Schliephake’s team. ’The advantage with this system is that it can be modularised,’ Schliephake explains. ’We can attach different growth factors with different complementary peptides to achieve variable degrees of hybridisation that should give us some control over the rate of release of the growth factor.’
Healing bone
In yet more severe cases of jawbone damage, such as where tissue has been excised due to diseases such as cancer, the bone itself needs to be repaired. At the Eastman Dental Institute, Anne Young’s team is developing novel materials to encourage the growth of new bone.
’The idea is that these are adhesive materials that will hold damaged bone together or fill a space in bone - for example where diseased bone in the jaw has been removed - and will allow the bone to regenerate,’ says Young. ’As the new bone grows the adhesive will biodegrade, eventually being replaced completely by the natural bone tissue.’

One system showing early promise is based on polylactide. ’We start with polypropylene glycol and attach short polylactide oligomers to this,’ she explains. ’Because the polylactide chains are relatively short, they remain fluid. We then incorporate methacrylate, which cross-links under blue light.’ Solid calcium phosphate particles are suspended in the liquid; to improve the mechanical strength of the material, help reduce the heat and shrinkage of polymerisation as the composite material sets and also nourish the growing bone when it is released as the adhesive biodegrades.
’The material now has the properties we need,’ Young says. ’It is biodegradable and it can set rapidly under a quick burst of blue light - within a few tens of seconds. As it degrades it releases the calcium phosphate, which is absorbed by the growing bone. Also the calcium phosphate helps to neutralise the acidity that is produced as the polymer degrades.’
Another attractive characteristic of the material is its ability to hold and release a variety of compounds. ’We have shown, for example, that we can add the antibacterial compound chlorhexidine, often found in mouthwash formulations, to the mix,’ Young says. ’We have also incorporated anti-inflammatories and larger biological molecules such as DNA. Because the adhesive sets so quickly the molecules it is carrying are not damaged to any significant extent by the generation of free radicals during polymerisation. We have also shown that it is possible to control the rate of release of these types of compound by changing the structure of the polylactide monomer. We have experimented with a number of polymer structures and have shown that some drugs are released quickly and others slowly. Generally, small drugs can slowly diffuse out of their surrounding solid matrix. With larger active components, the material must degrade before they can be released.’
Chemistry is not only playing a part in fixing damaged teeth and jaws, there is also a lot of work aimed at preventing damage in the first place. For example at Queen Mary, University of London, Paul Anderson is interested in the way that certain proteins in saliva serve to protect enamel against acidic demineralisation, and whether new analogues of these proteins can be engineered that could be used in novel formulations to protect teeth. One such protein is called statherin, which has been shown to play a role in reducing the dissolution of enamel. ’We know that statherin has calcium binding sites, and also hydroxyapatite binding regions,’ says Anderson. ’If you replicate the conditions of acid attack on tooth enamel in the test tube, and coat the enamel with statherin the dissolution rate drops by about half. We are working with colleagues in the US to try to understand the mechanism for this.’
It might even be possible, Anderson says, to develop therapeutic formulations based on these peptides for people who have medical and dental conditions that result in their having little or no flow of saliva and therefore lose the protective role of these salivary proteins.
Simon Hadlington is a freelance science writer based in York, UK





No comments yet