

Glucagon-like peptide-1 agonist drugs, such as semaglutide, could save countless lives at risk due to diabetes and obesity. Rachel Brazil looks at the difficulties in making the peptides themselves, and what’s coming next
It’s rare that the public becomes aware of a recently approved drug, but the chances are you’ve heard of semaglutide, or its tradename Ozempic, one of a growing number of drugs that replicates the action of the natural hormone, glucagon-like peptide-1. They’ve been widely covered in the global media as a much sought-after solution to losing weight. For some this is a matter of vanity, but for the estimated one billion people suffering from obesity in the world, it could prevent serious ill-heath and death.
GLP-1 is released in the gut in the presence of glucose and stimulates the release of insulin from pancreatic B cells, enabling fine control of blood sugar levels. The first drug targeting the GLP-1 receptor was exenatide, released in 2005 as a twice-daily injection to treat type II diabetes. It was discovered in the saliva of the Gila monster, a venomous lizard found in the American southwest, although no one knows why the lizard produces a molecule that replicates the action of GLP-1 when injected twice a day. For at least 20 years, pharma companies led by Novo Nordisk and Eli Lilly have been trying to find a better alternative. Novo was first to hit the jack pot with semaglutide, approved to treat diabetes in the UK in 2019 (as Ozempic).
The attention it is now receiving stems from its ability to promote weight loss more effectively than any previous drug therapy. In a clinical trial participants lost an average of 15% of their body weight after 68 weeks. Now production cannot keep up with demand for this instant blockbuster peptide drug, also marketed for weightloss as Wegovy, and the similar GLP-1 drug developed by Lilly, tirzepatide (Zepbound or Mounjaro). For pharma, the race is now on to ramp up and optimise production while developing the next generation of these drugs.
Early promise
The GLP-1 hormone is part of the intricate mechanism in our bodies to distribute glucose, but avoid the toxicity associated with high concentrations in the bloodstream. The 30-residue peptide regulates the release of insulin, but doesn’t stick around. ‘Its effects are so powerful that there are mechanisms that very quickly disable it,’ explains chemist Sam Gellman from the University of Wisconsin–Madisonin the US. The enzyme dipeptidyl peptidase 4 (DPP-IV) cleaves it between the second and third residues which renders it inactive within several minutes, and explains why GLP-1 cannot be used as a drug itself.
Efforts to synthesise a more chemically stable analogue resulted in the drug liraglutide, a daily injection for diabetics released by Novo Nordisk in 2015. Attaching a 16-carbon side chain (palmitic acid) to the peptide allowed the molecule to bind to the abundant blood protein albumin and keep it in circulation. By 2004, Novo had selected its new lead candidate from 217 peptides, which became the once weekly injection semaglutide. This variant incorporates an 18-carbon hydrophobic fatty acid side chain (1,18-octadecanedioic acid) to bind the peptide to albumin, which is akin to ‘attaching a house to GLP-1’, says chemist Krishna Kumar from Tufts University in Massachusetts, US.
The other crucial modification that increases its stability is substituting the eighth residue , an alanine, with amino-isobutyric acid (AIB) which has an additional methyl group making the alpha carbon quaternary. ‘Just that one small subtle substitution, enhancing the molecular weight by 14 daltons, substantially increased the stability of the the peptide,’ says Paul Levine, a chemist at peptide company Insamo in California, US. The change prevents DPP-IV cleaving the molecule, resulting in a previously unheard of half-life of a week. Novo has even been able to produce an oral formulation.
‘People report they’re just not that interested in food since they started taking drugs like semaglutide,’ says Stefan Trapp, a neuroscientist at University College London in the UK. He is trying to develop a greater understanding of this process and particularly the role of the brain. These drugs may have even broader therapeutic uses. A recent study shows people with obesity taking GLP-1 drugs are 20% less likely to suffer a cardiovascular event, and studies are under way for their use to treat the liver disease non-alcoholic steatohepatitis, as well as the neurodegenerative conditions Parkinson’s and Alzheimer’s. Plus there are indications it could even treat addiction.
Production problems
Anyone trying to get hold of these drugs will be aware of the recent shortages. There is huge demand, but producing peptide drugs in large quantities is proving a challenge for Novo and Lilly. Kumar says Novo insiders have told him the demand is about 20 times higher than the current supply. Semaglutide is made by recombinant expression of most of the peptide sequence in yeast, followed by several chemical modifications. The amino acid sequence is amended to switch a lysine for an arginine, leaving only one lysine in the sequence, which is used to introduce the fatty acid side chain. Then the first two amino acids including the AIB unit are also added.
For tirzepatide, approved in the UK in March, Lilly has opted for a chemical synthesis. The molecule consists of 39 amino acids, with the non-natural AIB incorporated at positions 2 and 13, which make it difficult to make using cheaper recombinant technologies. But the alternative chemical synthesis is not easy at scale. The solid phase peptide synthesis (SPPS) method attaches the first amino acid to a resin bead, with stepwise reactions to lengthen the chain. To prevent polymerisation of each added amino acid, its alpha amino group and reactive side chains are masked with a temporary protecting group. Between each stage the resin is filtered and washed to remove byproducts, excess reagents and the terminal protecting groups, and the cycle is repeated until the final peptide is cleaved from the resin and purified using chromatography.
With so many steps the process has a failure rate of about 20% for peptides above 30 amino acids, leaving a lot of impurities to remove. Purifying long peptides is difficult, plus these GLP-1 peptide drugs have been modified to include a fatty acid side chain, and ‘lipids themselves can be very difficult to purify, because they’re very hydrophobic, and tend to stick to the [purification] column,’ says Levine.
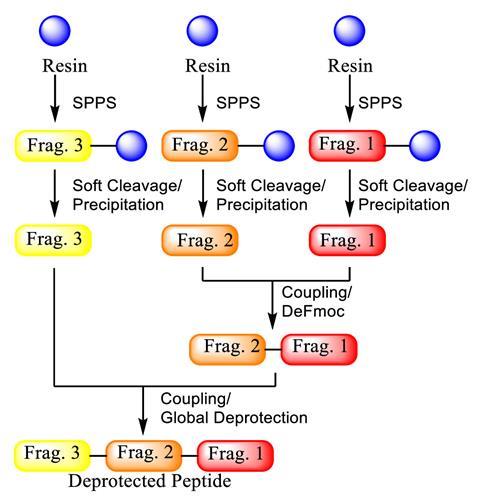
Lilly has gone for a hybrid method, outsourcing the manufacture of several peptide fragments and then assembling the fragments using liquid-phase peptide synthesis (LPPS). Instead of being bound to resin, the non-side-chain carboxyl functionality of the amino acid in the peptide fragment is protected as a bulky ester. Once reacted, a ceramic membrane is used as a nanofilter to separate based on molecular weight and hydrophobicity, removing smaller impurities and allowing further peptides to be coupled in the liquid phase. In a recent publication Lilly says the hybrid SPPS/LPPS method allows for high purities with a yield greater than 70%.
Both companies are increasing peptide production capacity. Novo Nordisk is spending $6 billion (£4.7 billion) on a new 170,000m2 facility at its Kalundborg site in Denmark to be completed in 2029. Along with other investments, Novo says it will ‘future-proof’ the company’s supply. Lilly recently completed a new hybrid peptide manufacturing facility at its existing site at Kinsale in Ireland, together with expansion in the US and Germany.
One important issue is how to make peptides in a greener way as well as at lower cost. SPPS uses large quantities of organic solvents – often five washes per step, which drives up the waste and environmental footprint for making peptides. Lilly has been investing in new technologies to improve the LPPS method by optimising the separation of the growing peptide chain. One method, known as molecular hiving, tags the first amino acid with long soluble hydrophobic anchor molecules, which can later be removed. The growing tagged peptides can be precipitated in aqueous solution and other impurities rinsed away before the next cycle starts. Overall the process uses fewer reagents and solvents.
The race to generics and alternatives
Novo Nordisk’s first GLP-1 drug liraglutide will be off patent in November and in June Teva Pharmaceuticals received US authorisation to market the first-ever generic version, to treat diabetes. Other companies are following suit. Pharmaceutical chemist Walter Cabri from the University of Bologna in Italy says many generics companies are working on full chemical syntheses of liraglutide. The other big prize will be semaglutide, which goes off-patent in Europe in 2031
We are working on the hybrid synthesis
Cabri is a consultant for the intravenous generic drug company Fresenius Kabi, and is working with it on novel peptide production methods. He says companies need to find methods that give them freedom to operate – that are not under patent to other companies. ‘We are working on the hybrid synthesis, where we make some [peptide] pieces with SPPS and then we will couple [them] together with an enzyme.’ So far they have done this for liraglutide using a unique ligation point – the site where the enzyme couples two natural amino acids.
Others are looking at alternative ways to stabilise GLP-1 drugs that might prove easier to produce. Akhter Hossain at the University of Melbourne in Australia has suggested rather than adding a fatty acid side chain, a glycan group may work instead – which is more hydrophilic and therefore easier to dissolve and purify. ‘In vivo, it is not actually going to bind to albumin, but [the glycan] has sialic acid moieties, which also reduces the liver metabolism, and thus increases the circulating half-life in the blood,’ explains Melbourne researcher Chaitra Chandrashekar, who carried out the work.
They were able to do the synthesis by joining just two peptide fragments with an enzyme, omniligase-1, which catalyses amide bond formation, using fewer steps than most other methods. Chandrashekar found the increase in yield was 10-fold. ‘We did use the same protocol to also make semaglutide; however, we could isolate only 4% of it, while we could isolate almost 45% of our glyco GLP-1.’ Rat studies show blood glucose lowering effects similar to semaglutide, although the half-life is not yet established. If it does compare favourably this might provide the kind of production boost that is going to be needed.
Multiple targets
The next generation of GLP-1 drugs is already entering the clinic – with a shift to dual and triple agonists. Drugs able to activate a number of receptors seem to perform better. Already authorised, Lilly’s tirzepatide targets both GLP-1 and the glucose-dependent insulinotropic polypeptide (GIP) receptor, which has a complementary role in stimulating insulin secretion and reducing appetite.
Lilly is following this with retatrutide, a triple agonist, which has completed phase 2 trials for treating obesity and cardiovascular disease. It additionally targets the glucagon (GCG) receptor, another part of the machinery to control blood glucose levels in line with energy expenditure. A recent trial comparing tirzepatide to semaglutide showed a greater increase in weight loss after a year, with losses of 15.3% with tirzepatide compared with 8.3% for semaglutide. Lilly’s phase 2 retatrutide trial achieved up to 17.5% mean weight reduction at 24 weeks.
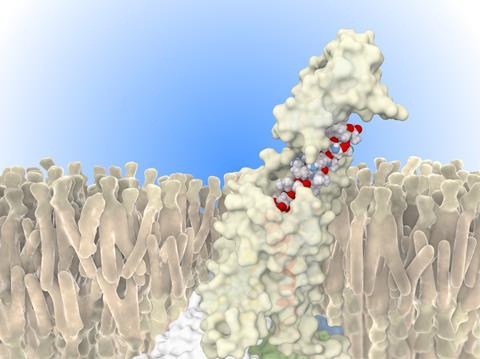
Using one molecule to target all these receptors seems to work because their structures are all based on similar long alpha helices. ‘If you squint and look at these receptors, they all look essentially identical, with small changes,’ says Kumar. The strategy is then to mix and match amino acid residues from the three natural peptides, ‘I call this a Frankenstein strategy, you’re taking the pieces from here, pieces from there,’ says Gellman.
Modifications are also being designed to create biased agonists. ‘When you activate the receptor, a lot of proteins bind to it intracellularly, but if you bind and only recruit the protein that you want, it can go through a more selective pathway,’ explains Levine. This is one strategy for reducing the nausea side effects which are commonly experienced with GLP-1 drugs. With the GLP-1 receptor there is the pathway linked to insulin control, but also a pathway that recruits the signalling molecule beta arrestin, which causes the side effects but also results in the whole receptor and drug molecule being taken inside the cell, shutting down any further activity. The challenge is to bias the receptor response and so reduce these competing signalling mechanisms.
There’s going to be an explosion in the sheer number of compounds
Kumar has found he can design bias into GLP-1 analogues by simply alkylating or trifluoroalkylating the N-terminal amino acid using an alkyl halide. He has created a library of DPP-IV resistant peptides that bind at the receptor sites. ‘We have unimolecular, dual agonist, tri-agonist, [and] tetra-agonists, where you can just add an alkyl group, and then you can tune GLP-1 receptor [sensitivity] up or down,’ says Kumar. You can do the same thing with GIP, GCG and peptide tyrosine tyrosine, which also play a role in appetite suppression.
Ultimately it may turn out that different molecules may suit different patient populations and different conditions. ‘It may be true that what is good for glucose homeostasis or what is good for losing weight may not be the best thing for chronic kidney disease,’ suggests Kumar. ‘There’s going to be an explosion in just the sheer number of compounds and also the methods to make them.’
A hybrid approach
Gellman has taken a different approach to novel GLP-1 drugs based on his synthetic beta peptides. These are made by substituting some natural alpha amino acids with beta amino acids, that have the amino group attached to the beta carbon two atoms away from the carboxylate group. These artificial peptides or ‘hybridtides’, can form the same alpha helical structures as GLP-1, but are resistant to protease degradation. Gellman’s company Longevity Biotech now has a drug candidate that activates both GLP-1 and GIP, is biased towards the insulin signalling pathway and can be orally formulated.
In his latest work Gellman has started to examine more closely how the membrane-anchored receptors engage with these drugs. He has found that a hybridtide with a kink near its end is able to wiggle between a helical and non-helical conformation within the receptor (both conformations being observed using cryo-electron microscopy). In doing so the molecule is constantly docking and undocking and lengthening the drug’s action. ‘I think most people think about these processes in terms of a single, ideal bound conformation of the peptide to the receptor as the basis for signalling,’ says Gellman, ‘but I’m increasingly suspecting that certain modes of dynamics are critical for signalling.’ He is now trying to design this structural variability into his hybridtides to see if this will improve on the performance of GLP-1 drugs.
Getting to the brain
Trapp is working to fully understand how GLP-1 drugs work is still ongoing, particularly whether these peptide molecules penetrate the brain. A lot of clinicians think they do, but he is not persuaded. Rather, he thinks their ability to reduce appetite occurs by stimulation of parts of the brain that sit outside the blood–brain barrier – the selective semi-permeable membrane that keeps most large molecules out. His experiments with fluorescently labelled GLP-1 agonists prove this.
I was among the people who thought five years ago there’ll never be small molecules here
There are GLP-1 receptors and a second source of GLP-1 within the brain, completely isolated from the peripheral system and Trapp has shown that stimulating these receptors can have an even greater impact on weight loss in animal studies. Getting into the brain might also be important to treat neurodegenerative diseases where there are some promising results suggesting they slow disease progression. But targeting GLP-1 receptors in the brain will likely need a small molecule drug.
In fact several pharma companies already have small molecule GLP-1 agonists in their pipelines. ‘Frankly, I was among the people who thought five years ago, there’ll never be small molecules here, because the site you’ve got to bind is just too big,’ says Gellman, but he concedes it looks like he was wrong. In 2023 Lilly published results of its phase 2 trial for orforglipron, a once-daily oral drug which achieved up to 14.7% mean weight reduction at 36 weeks, and Pfizer has completed phase 2 trial for its oral drug danuglipron and is now optimising the formulation.
If these oral small molecule drugs can match their larger cousins, they may solve the problem of the difficult mass production of peptide drugs. In the meantime, there has also been the first attempt to create a gene therapy that could integrate a GLP-1 secreting transgene directly into pancreas beta cells. In 2023, Fractyl Heath announced mice given semaglutide and treated with its gene therapy Rejuva, administered directly to the pancreas, had maintained a 22% weight loss for 28 weeks after stopping the drug and performed better than those given only semaglutide.
However the field develops, Trapp says the control of weight through GLP-1 is a genuine game-changer. ‘Compared to what we had before, if we had weight loss of about 5%, that was a real success. Now, with these drugs, we’re looking at 15%, and possibly even more.’
Rachel Brazil is a science writer based in London, UK













1 Reader's comment